The biggest complication for any brain or spinal cord surgery is the damage to neural structure during the surgical procedure. Surgical insults account for app 50% of post operative neurological deficits as showed by statistics.

Intraoperative neuromonitoring is becoming prevalent now a days to avoid such risks. For any spinal cord surgery the neurological deficit arise during surgery due to ischemia or mechanical injury caused during surgery. If by any means the operating surgeon can be warned regarding such insults , this can definitely reduce the chance of such deficits.
PURPOSE OF IONM
- Reduce the risk of postoperative neurological deficits as much as 50% as evidenced by studies
- Identify specific neuronal structures and landmarks that cannot be easily recognized
- Research purposes in basic science, pathophysiology and therapeutic management
What are the electrophysiological studies performed as a part of IONM?
- Motor Evoked Potentials - detects surgical insults to the ventral part of the spinal cord
- Somatosensory Evoked Potentials - detects surgical insults to the dorsal part of the spinal cord
- Free run Electromyography - monitor selective nerve root functions
- Triggered EMG - used to monitor individual pedicle screw placement alignment
A combination of all the above mentioned studies known as COMBINED MULTIMODALITY
IONM yield almost 100% specificity and sensitivity.
The purpose of IOM is to detect
response changes due to surgery, not to make a clinical diagnosis
SOMATOSENSORY EVOKED POTENTIALS - SSEP
Stimulation of peripheral nerves and recorded from the scalp. It monitors the dorsal column of the spinal cord. They directly monitor dorsal column medial lemniscal pathways. They do not directly monitor corticospinal activity.
ALARM CRITERIA
- 50% reduction in amplitude
- 10% increase in latency

TRANSCUTANEOUS MOTOR EVOKED POTENTIALS - TcMEP
• Stimulation
through the skull with signal recording at the level of
- muscle (CMAP)
- nerve (neurogenic MEP)
- spinal cord ( D-wave )
- Allows assessment of entire motor axis including motor cortex, corticospinal tract, nerve root and peripheral nerve
- Sensitivity of 100% when monitoring 6 sites, compared to sensitivity of 88% when monioring only 2 sites (Langeloo et al, 2003)
INTERPRETATION
- ALL OR NOTHING CRITERIA - the most used method,complete loss of the MEP signal from a baseline recording is indicative of a significant event
- AMPLITUDE CRITERIA - 80% amplitude decrement in at least 1 out of 6 recording sites
- THRESHOLD CRITERIA - increases in the threshold of 100 V or more required for eliciting CMAP responses that are persistent for 1 h or more
- MORPHOLOGY CRITERIA - changes in the pattern and duration of MEP waveform morphology

FREE RUN EMG
• Widely
used for monitoring selective nerve root function during spinal cord surgery
• During
spinal cord instrumentation and pedicle screw placement, postoperative radiculopathy is more likely than SCI, making spontaneous EMGs optimal
• No
stimulations required
• Continuous
recordings made
• One
muscle group per nerve adequate
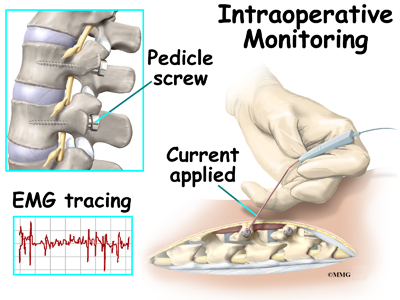
TRIGGERED EMG ( PEDICLE SCREW STIMULATION)
• Used
to determine whether screws have breached the medial or inferior pedicle wall
and thus pose a risk to the exiting nerve root at that level
• When
a pedicle screw is accurately placed, the surrounding bone acts as an insulator
to electrical conduction, and a higher amount of electrical current is thus
required to stimulate the surrounding nerve root.
• When
a medial pedicle wall breach occurs, the stimulation threshold is significantly
reduced
COMBINED MULTIMODALITY IONM
• Standard
practice
• Combination
of monitoring techniques – SSEP, MEP, Triggered EMG and Free run EMG
• Sensitivities
and specificities reaching almost 100%
After these basics of all the techniques, it is very important to understand the drawbacks too. For example we need to take an average of many readings for SSEP. Hence following an acute insult, change in SSEP is seen after quite some time and by that time there are possibilities of irreversible neurological changes .According to Hillibrand et al in 2004, SSEP changes lag behind MEP changes by an average of 16 minutes. SSEP have a very low sensitivity in detecting individual nerve root damage which is more prevalent in spinal instrumentations. There are so many minute things to be taken into consideration while performing IONM.
It is very important to identify true positive and false positive changes and to report at the right time. Considering other factors like anesthetic agents used, hypothermia, hypovolemia, electrical interference etc and performing all trouble shooting and then coming to a conclusion and that too fast and perfect enough to avoid neurological insult
It was just yesterday that I was speaking to one of the Physiotherapist a very enthusiastic girl who wanted to work hard in the field of IONM. But was very depressed because of the reply she got from her hospital authorities that IONM IS A TECHNICIAN JOB. WE DONT NEED A PHYSIOTHERAPIST TO DO IT.
I have only one answer to this ruthless comment. It is mandatory to have a thorough knowledge of anatomy, physiology, orthopedics, surgery and electrophysiology before one begins with IONM. If it was any technician's job to do it, then even that technician needs this accurate training. Comparing the performance of a technician and a physiotherapist even for training in IONM, a physiotherapist will definitely stand apart and unique and shine out and complement the SURGICAL TEAM very well. If a consultant is not considering a technician worth to interprete EMG/NCV studies independently, how will a surgeon consider a technician interpret IONM results per operative?
People under estimating a trained Physiotherapist for IONM must definitely try and compare the efficiency of a technician versus a trained Physiotherapist and then take a decision by themselves.
JUST BECAUSE FEW CORPORATES ARE IN A PAY CUT POLICY EXPLOIT PHYSIOTHERAPISTS WITH SUCH POLICIES. FOR THEM IONM IS JUST AN INSTRUMENT TO SHOW.....NOT AN ETHICAL TECHNIQUE TO PERFORM.....OTHERWISE IF TECHNICALLY AND ETHICALLY PERFORMED IT SURELY NEEDS A VERY WELL TRAINED AND EFFICIENT ELECTROPHYSIOLOGIST
Whether a Physiotherapist performs IONM or someone else, most important is proper training, well experienced under thorough senior and aptitude to perform. A PERSON WITHOUT KNOWLEDGE OF EMG/NCV STUDIES CANNOT PERFORM IONM. Basic Certification and knowledge of EMG/NCV studies is mandatory. This is what ETHICS say. Manipulation knows no boundaries and inhumanity has no extent.
No comments:
Post a Comment